The Adherence Paradox: A System Designed to Fix Breakdowns, Not Prevent Them
Why the current healthcare system is structurally optimized for reactive intervention rather than proactive adherence — and what it would take to shift the default.
The healthcare system is remarkably good at responding to crises. It is far less good at preventing them — especially when the failure mode is something as quiet and invisible as a patient not taking their medication.
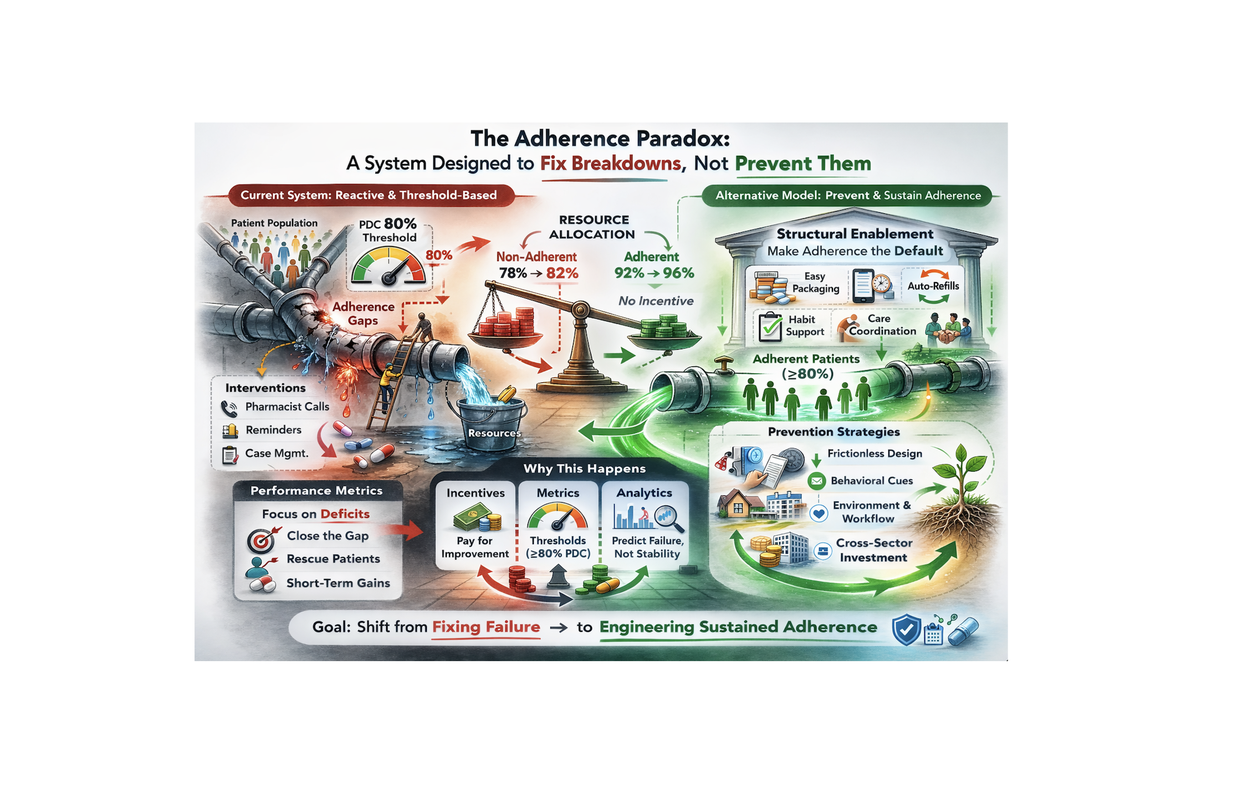
This is the adherence paradox: the system is designed to fix breakdowns, not prevent them. Incentives, metrics, and resources are concentrated at the point of failure — the ER visit, the hospitalization, the preventable complication — rather than at the upstream moment where the failure began: a patient who stopped taking their medication.
"The current system focuses resources on the 78–82% non-adherent patients who generate costs, rather than on making adherence the structural default for everyone."
How the Current System Works
The current model is reactive and threshold-based. Pharmacist calls, reminder programs, case management, and care coordination are all triggered after a patient has already shown signs of non-adherence — a missed refill, a gap in PDC, a hospitalization. The performance metrics reinforce this: close the gap, rescue the patient, short-term gains.
This approach has a structural problem: it allocates resources to the patients who have already failed, rather than preventing failure in the first place. And because the interventions add friction — log this, reply to that, enroll here, navigate a chatbot — they often select for patients who were already most likely to adhere.
The Alternative: Make Adherence the Structural Default
A prevention-first model looks different. Instead of waiting for failure, it invests in structural enablement — making adherence the path of least resistance from day one. Easy packaging. Habit support. Frictionless workflow. Auto-refills. Care coordination that activates before the gap, not after.
The goal shifts from "close the gap" to "prevent the gap." From "rescue the patient" to "set the patient up to succeed." From short-term gains to sustained adherence.
This is where packaging becomes strategic infrastructure, not just a container. The bottle is the one tool patients interact with every single day. If it makes the right action obvious — without requiring extra steps, extra devices, or extra willpower — adherence becomes easier by default.
Why This Matters for Pharmacies
For pharmacy leaders, the adherence paradox has a practical implication: the current model of intervention is expensive, labor-intensive, and largely reactive. Every pharmacist call, every outreach program, every case management touchpoint is a cost that could be reduced if the upstream failure rate were lower.
Shifting to structural enablement — packaging that makes adherence easier, workflows that support habit formation, dispensing systems that reduce friction — is not just a patient experience improvement. It is an operational efficiency play. Fewer interventions needed downstream means lower cost per adherent patient.
"We don't need another adherence program that asks patients to do more. We need the default bottle — used billions of times a year — to finally do its job and help patients succeed."
The Goal: Shift from Fixing Failure to Engineering Sustained Adherence
The adherence paradox is not a mystery. It is a structural consequence of how incentives, metrics, and resources are currently aligned. Changing it requires changing the default — not just adding more programs on top of a system that is already optimized for the wrong outcome.
RedCap is built on this premise: that the most powerful adherence intervention is not a new program, but a better default. A bottle that makes taking medication easier than not taking it. A dispensing system that supports habit formation without adding labor. An infrastructure that shifts the baseline — so that sustained adherence becomes the expected outcome, not the exception.
Next Article