Adherence Insights
Research, analysis, and perspective on medication adherence, pharmacy economics, and the behavioral science of habit formation.
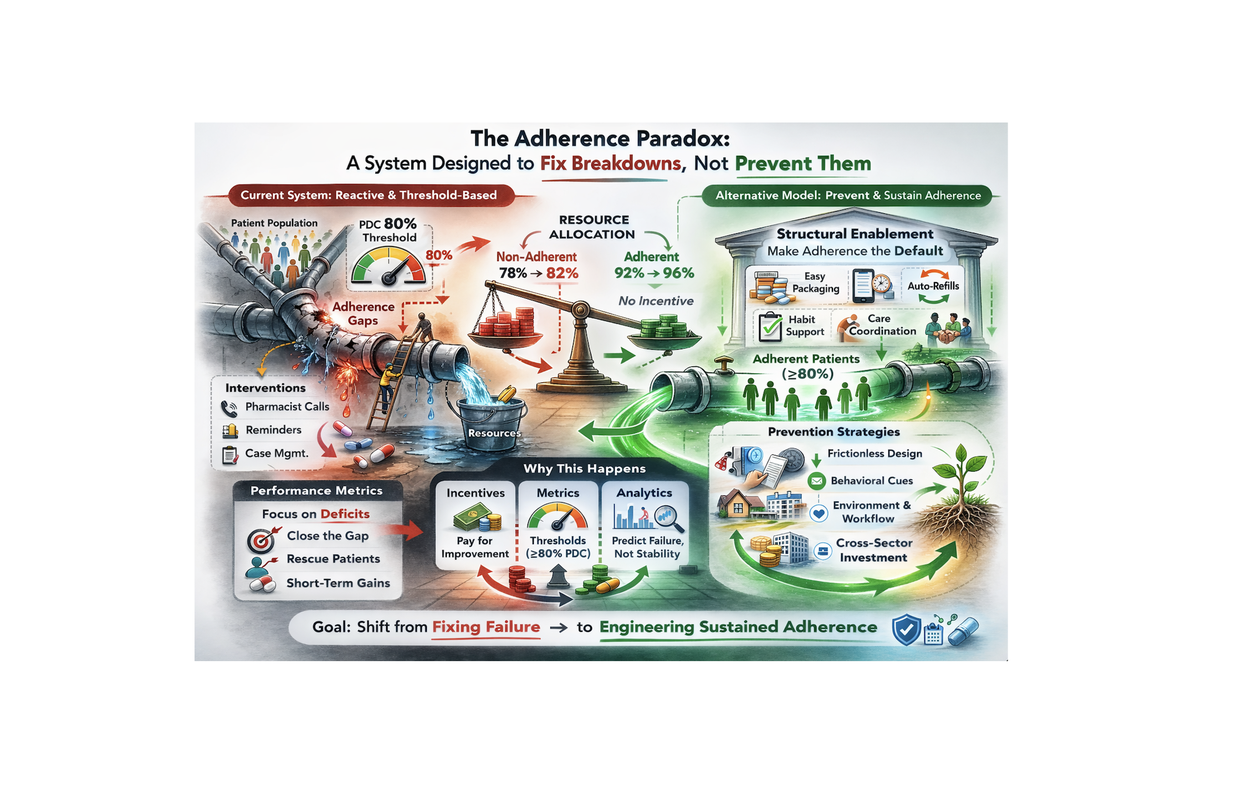
The Adherence Paradox: A System Designed to Fix Breakdowns, Not Prevent Them
The healthcare system is remarkably good at responding to crises. It is far less good at preventing them — especially when the failure mode is as quiet and invisible as a patient not taking their medication.
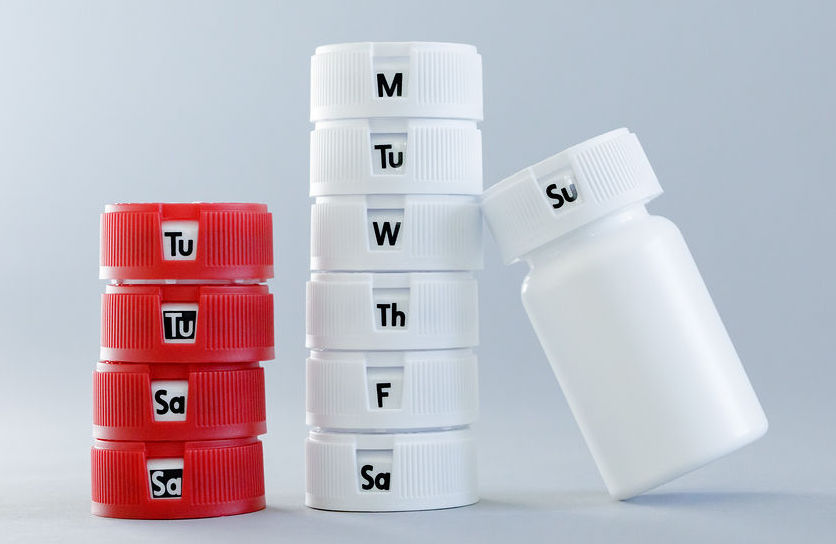
Text Messages Don't Build Habits. Packaging Does.
Pharmacies don't have an 'adherence education' problem. They have an execution problem that shows up downstream as refill gaps, avoidable service friction, and lower long-term retention.
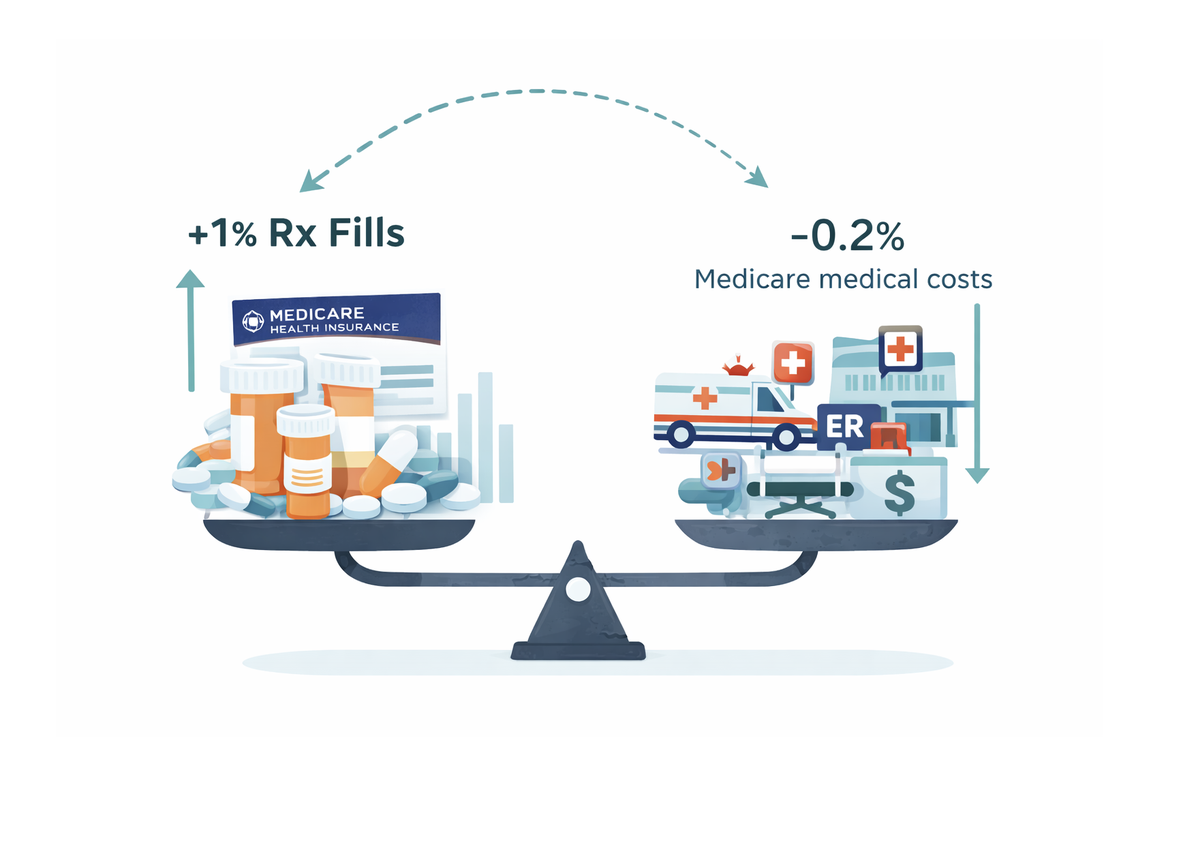
Medication Adherence Math
Everyone agrees that better medication adherence is good for patients. But how good is it economically? The Congressional Budget Office has a clear answer — and the numbers are staggering.
![[Non]-actions Speak Louder Than Words](https://d2xsxph8kpxj0f.cloudfront.net/310519663383179352/NskFZAWtgskE56NADUi3Bv/non_actions_today_number_831d6221.webp)
[Non]-actions Speak Louder Than Words
135,000 papers on medication adherence written between 1970 and 2020. And yet the standard bottle hasn't changed. Here's why — and what it takes to break the cycle.
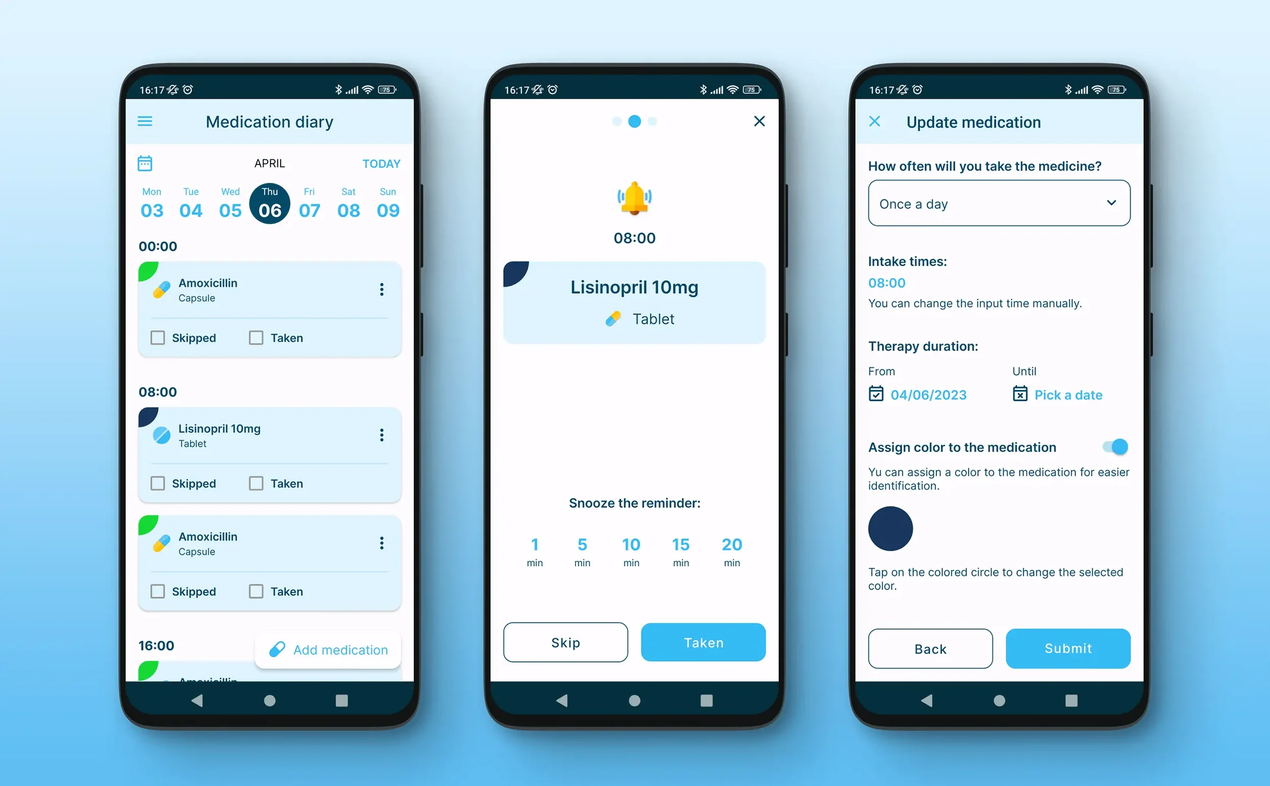
We Keep Trying to "Fix" Medication Adherence With More Text Messages and Apps
A major randomized pragmatic trial of 9,501 patients suggests that even thoughtfully designed text reminders don't move the needle on adherence. Here's what the evidence shows — and what to do instead.

Having Medication Is Not the Same as Taking Medication
The Wall Street Journal documented how automated refill systems create confusion and waste. The real problem: we've optimized for delivery, not for outcomes. Delivery is table stakes — outcomes are the differentiator.

We Optimized Pill Bottles for Toddlers, Not Patients
For more than 50 years, the U.S. prescription bottle has been treated as dispensing infrastructure, not a behavioral support system. The PPPA solved child poisonings — but created no parallel requirement to help patients stay on track.